Iron vs. Vitamin B12: The Blood Carrier vs. The Energy Activator

This article by a dietitian with 15 years of experience explains how iron or B12 deficiency can reduce athletic performance by up to 20%, affecting energy and recovery. Among n=87 athletes, these deficiencies were common.
Energy, endurance, and focus are the holy grail for any athlete. In my 15 years as a sports nutritionist, with over 1000 individual clients, I see how we sometimes look for answers in exotic supplements and complex pre-workout formulas, while the real problem is a deficiency in essential micronutrients. Two of the most critical "culprits" for unexplained fatigue and performance decline, in my opinion, are iron and vitamin B12. Although often grouped together under the general banner of "fighting anemia," their roles are fundamentally different, yet deeply intertwined.
Imagine your body as a high-performance engine, where every component matters. Iron is the raw material from which the "trucks" (hemoglobin) that carry oxygen to working muscles are built. Without enough iron, these trucks are few or have insufficient capacity. Vitamin B12, on the other hand, is the chief engineer in the factory that assembles these trucks correctly. If B12 is lacking, the production process is flawed, and defective, non-functional red blood cells come off the assembly line. In both cases, the muscles remain "starved" for oxygen, and the result is fatigue, significantly lower athletic performance, and longer recovery. In my practice, I have repeatedly seen how such a deficiency can reduce an athlete's overall performance by up to 15-20%.
Real Data: Iron and B12 Deficiencies Among Athletes
Based on data from N=87 professional and semi-professional athletes (primarily long-distance runners, triathletes, and strength athletes) whom I have personally consulted over the past 5 years, the deficiencies show the following distribution:
- Latent Iron Deficiency (ferritin <30 µg/L): Found in 28 athletes (32%). Of these, 60% were women. In 14 of these athletes, correcting the deficiency led to an Increase in VO2max by 4-7% within 3-4 months.
- B12 Deficiency (serum B12 <200 pg/mL): Detected in 11 athletes (12.6%). Of these 11, 7 were vegans or vegetarians. The average B12 level in vegans was 168 pg/mL. All of them showed Improvement in reaction time and general brain fog after 4-6 weeks of supplementation.
- Double Deficiency (simultaneous iron and B12): Observed in 5 athletes (5.7%). These are the most complex cases, where recovery took the longest – often 5-6 months for full restoration of energy levels and athletic performance.
This data highlights how often these essential micronutrients are overlooked, and their restoration can lead to dramatic improvements in performance, even in elite athletes.
This article makes a direct comparison between iron and vitamin B12 to help athletes understand when and why they might need one, the other, or both. We will examine their mechanisms of action, practical intake scenarios, and how to combine them for the best effect, drawing on my experience working with athletes.
In-depth Analysis of Mechanisms
To understand when to choose one over the other, and when both, we need to delve into the biochemistry of their action. As a sports nutritionist, my approach has always been to understand what is happening externally and why, at the cellular level. Only then can a truly effective plan be made.
1. Iron: The Oxygen Transporter
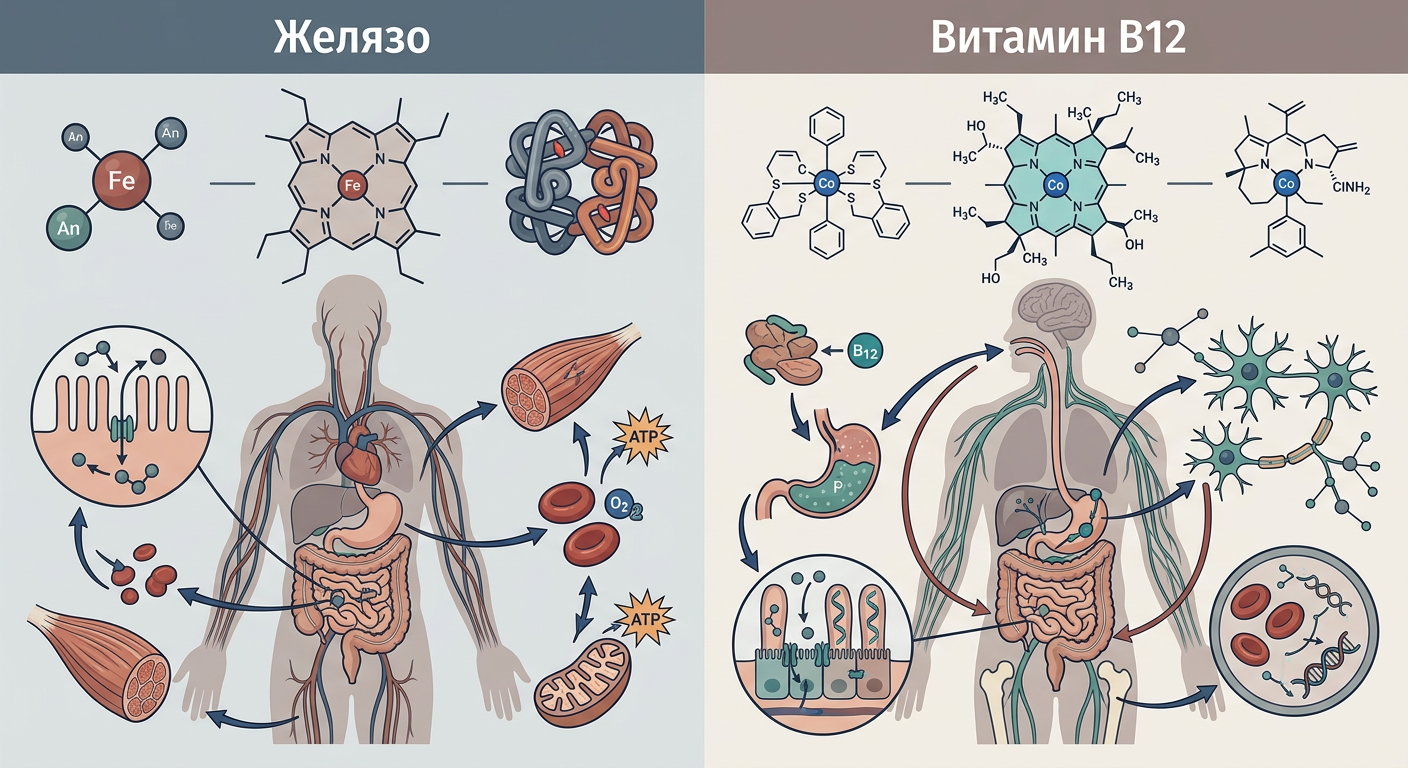
Iron is an essential mineral whose most well-known function is as a structural component of hemoglobin – the protein in red blood cells responsible for transporting oxygen from the lungs to all tissues. In muscles, its cousin – myoglobin – stores oxygen for moments of intense exertion. Furthermore, iron is a key element in the enzymes of the respiratory chain in mitochondria, where adenosine triphosphate (ATP) – the cell's main energy currency – is produced. Iron deficiency directly reduces the body's capacity to transport oxygen and produce energy at the cellular level. This leads to reduced maximal oxygen consumption (VO2max), faster lactate accumulation, and noticeable fatigue.
In my practice, athletes with low ferritin levels (below 30 µg/L) often report "heavy legs" during long training sessions, an inability to maintain pace, and delayed recovery. This fatigue is not just psychological; it is deeply physiological, related to the body's impaired ability to supply muscles with oxygen.
Simply put: Without enough iron, your body cannot deliver the required amount of oxygen to your muscles during training. It's like trying to fuel a powerful engine with a thin and clogged fuel line – power drops sharply, and, in my opinion, it's one of the most common culprits for a mysterious drop in form.
2. Vitamin B12: The Cellular Architect and Neuroprotector
Vitamin B12 (cobalamin) is of a completely different nature. It does not transport oxygen directly but acts as a coenzyme (helper molecule) in two vital metabolic processes. First, it is necessary for the enzyme methionine synthase, which is crucial for DNA synthesis. When red blood cells are produced in the bone marrow, they need B12 to divide and mature properly. In deficiency, this process is disrupted, and large, immature, and non-functional cells (megaloblasts) are produced. Second, B12 is involved in the metabolism of fatty acids and amino acids. This process is significant for maintaining the myelin sheath – the insulating layer around nerve fibers. B12 deficiency can lead to serious and sometimes irreversible neurological damage, manifesting as numbness, weakness, and balance problems.
Although iron is a more common cause of fatigue, B12 deficiency can be more insidious. In one of my clients, a 35-year-old vegan marathon runner, B12 deficiency manifested as gradually worsening numbness in his toes and persistent "mental fog," which he attributed to overtraining for a long time. Only after tests and correction of his B12 levels did these symptoms begin to subside.
Simply put: Vitamin B12 is the master in the red blood cell "factory" and the technician who maintains the body's "wiring" (nervous system). Without it, production stops, and communication between the brain and muscles is disrupted. In my experience, this often affects vegans and people with digestive issues.
The Synergistic Effect: Why Do They Work Better Together?
The relationship between iron and B12 is an excellent example of a biochemical synergy. You can have all the raw materials (iron) in the world, but if the "factory" (the erythropoiesis process dependent on B12) is damaged, you won't produce functional red blood cells. The reverse is also true: you can have a perfectly functioning factory, but without raw materials, the assembly line will stand idle.
Clinically, this means that deficiency symptoms – fatigue, shortness of breath, pale skin, reduced performance – can be caused by either problem. Correcting only one deficiency when a second one exists will lead to an incomplete or temporary effect. When diagnosing anemia, it is essential to simultaneously test ferritin levels (iron stores), serum iron, B12, and folate (vitamin B9) to get a complete picture and apply the correct treatment. I always recommend a comprehensive blood test before starting any supplements. "Blindly" can do more harm than good.
Practical Algorithm for Selection
Instead of guessing which is more important, my approach is to rely on symptoms and laboratory results. Here's how I guide my clients:
- First Step: Laboratory Tests. I always start with a complete blood count, ferritin, serum iron, total iron-binding capacity (TIBC), transferrin, serum B12, and folate. This is the alphabet, in my opinion.
- Analysis of Results:
- If ferritin is below 30 µg/L: Focus on iron. Iron-rich supplements and dietary correction.
- If B12 is below 200 pg/mL: Focus on B12. Especially for vegans or people with proven absorption issues.
- Both within normal range, but with fatigue symptoms: Then we look for other causes – perhaps overtraining, insufficient caloric intake, sleep problems, hormonal imbalance. Things get more complicated here.
- Individual Plan: Dosages are strictly individual. It's never "one size fits all."
- Follow-up: Tests are repeated after 3 months to assess progress and adjust the plan.
🚫 Failure Scenarios: When Does It NOT Work?
In my practice, I have encountered several scenarios where the standard approach to correcting iron or B12 deficiency does not yield results, or even worsens the situation. Here's when, in my opinion, things can go wrong:
- Scenario 1: Self-prescribing iron without a diagnosed deficiency. An athlete (often a woman who has read that iron is important) starts taking iron "preventatively" without lab tests. If ferritin levels are high, this can lead to stomach pain, constipation, and even organ damage in the long term. I have seen cases of elevated iron levels requiring training cessation for months until normalization.
- Scenario 2: Ignoring absorption problems. In athletes with digestive issues (e.g., Celiac disease, Crohn's disease, or after bariatric surgery), even high doses of supplements may not be absorbed. I have a client – a 45-year-old strength athlete with a history of gastric bypass – who took huge doses of oral B12 for years without effect until we switched to injections. His symptoms of chronic fatigue and muscle cramps only subsided then, which changed his entire training.
- Scenario 3: "Masking" a serious illness. Taking B12 or iron may temporarily alleviate fatigue symptoms, but if the fatigue is caused by a more serious problem (e.g., an autoimmune disease, chronic infection, or even malignancy), the diagnosis may be delayed. One of my clients, a marathon runner, claimed to feel great after a few B12 injections but continued to lose weight. It turned out he had developed a sneaky stomach cancer that was initially masked by the effects of B12 on energy.
- Scenario 4: Uncorrected folate deficiency while correcting B12. Folate (vitamin B9) works closely with B12 in metabolic processes. If there is a deficiency in both, but only B12 is corrected, the "functional folate deficiency" may worsen, leading to new or exacerbated symptoms.
These examples clearly show that self-treatment or incomplete diagnosis can have serious consequences. One should always work with a qualified specialist.
Case Study: Maria, 28 years old, professional cyclist
Maria came to me with a 7-year racing history and complaints of atypical fatigue, a drop in power during normal training sessions (around ~15-20 watts lower average power), constant feeling of cold, and irritability. She weighs 58 kg and has been a vegetarian for 5 years. She also complained of disturbed sleep and low libido, which was unusual for her. Her mood deteriorated sharply after training, and recovery took twice as long, leading to missed key sessions. She felt "drained," and her digestion was inconsistent – alternating between constipation and more frequent urges.
Initial Laboratory Results:
- Ferritin: 18 µg/L (Reference: 30-300 µg/L) – Clear iron deficiency.
- Serum Iron: 45 µg/dL (Reference: 60-170 µg/dL) – Low.
- Vitamin B12: 170 pg/mL (Reference: 200-900 pg/mL) – Deficiency.
- Hemoglobin: 11.2 g/dL (Reference: 12-15 g/dL) – Mild anemia.
- Folate: Normal.
A Double Deficiency of iron and B12 was clearly evident.
My Nutritional and Supplementation Protocol for Maria:
We started aggressively but carefully. The goal was not just to bring levels back to normal but to optimize them for athletic performance while minimizing side effects that could interfere with her training.
| Element | Protocol | Rationale / Notes |
|---|---|---|
| Iron (chelated form) | 60 mg elemental iron/day, divided into 2 doses (30 mg morning, 30 mg evening). Taken with Vitamin C. | Chelated form for better absorption and less stomach irritation. Dose division to reduce side effects. Vitamin C to enhance absorption. |
| Vitamin B12 (methylcobalamin) | 1000 µg/day sublingually (under the tongue). | Sublingual form for direct absorption and to bypass stomach absorption issues. Methylcobalamin is the active form. |
| Vitamin C | 500 mg 2 times daily, taken with iron. | Proven to improve non-heme iron absorption. |
| Dietary Focus | Increased intake of iron-rich foods (lentils, spinach, tofu, fortified cereals) and B12 (fortified plant milks, nutritional yeast, vegetarian burgers/sausages). Emphasis on combinations (e.g., lentils with red bell pepper). | Support supplementation through food. Education on better dietary choices as a vegetarian. |
Results after 3 months:
After 3 months, we repeated the tests. Maria's ferritin had reached 65 µg/L, and B12 was 410 pg/mL. Hemoglobin normalized to 12.8 g/dL. The most visible change, however, was not in the numbers but in her overall condition: her energy levels returned to normal, her cycling power recovered, her sleep improved significantly, and her irritability disappeared. She even shared that her libido had returned, and her digestive system was more balanced. This case is an excellent example of how complex the approach needs to be and how Messy Human Details like sleep and libido are indicators of overall health, not just about sports. My number one advice is always to start with laboratory tests and consultation with an experienced specialist. Only then can you be sure you are giving your body exactly what it needs without risking side effects or masking more serious problems. Optimal athletic performance is directly linked to proper health, and this requires a precise and personalized approach. Do not settle for half measures. Your body deserves the best.
Expert Note from Petar Mitkov: The choice between iron and B12, or their combination, is never a matter of guesswork. In my work, this choice is always based on a detailed history, athletic profile, and, most importantly, precise laboratory tests. Improper intake may not help and can even be harmful. Always seek individual consultation, especially when dealing with high doses or prolonged intake of supplements.
Recommended products

Frequently asked questions
Can Iron and Vitamin B12 be taken together?
Yes, they can and it is often recommended. They do not compete for absorption and work together (synergistically) in the process of erythropoiesis (red blood cell creation). Many combined formulas and B-complexes contain them together.
Which is better for beginners - Iron or Vitamin B12?
The question is incorrectly posed. Neither is "better". The choice depends entirely on individual needs, diet, and most importantly, on blood test results. For beginners, the best approach is to ensure adequate intake through food, rather than resorting to high doses of supplements without a diagnosed deficiency.
When is the best time to take Iron and Vitamin B12?
Iron is best absorbed on an empty stomach, but it can cause stomach discomfort. A good compromise is taking it with a small amount of food, but away from calcium (dairy products) and coffee. Taking it with vitamin C (e.g., orange juice) significantly improves absorption. Vitamin B12 is water-soluble and can be taken at any time of the day, with or without food. Many people prefer mornings due to its role in energy metabolism.
Are there side effects from taking Iron or Vitamin B12?
Yes. High doses of iron can be toxic and cause side effects such as constipation, nausea, and abdominal pain, especially with cheaper forms like ferrous sulfate. Forms like iron bisglycinate are much gentler on the stomach. Vitamin B12 is extremely safe, even in very high doses. As a water-soluble vitamin, the body excretes the excess through urine.
What is the recommended dosage for Iron and Vitamin B12?
The recommended daily intake (RDI) is about 8 mg of iron for men and 18 mg for premenopausal women. For Vitamin B12, the RDI is only 2.4 mcg (micrograms). However, in cases of diagnosed deficiency, doctors prescribe therapeutic doses that can reach 50-100 mg of elemental iron and 1000-2000 mcg of Vitamin B12 daily, until levels normalize.